Dilger, Hansjörg (2012). The (Ir)Relevance of Local Knowledge: Circuits of Medicine and Biopower in the Neoliberal Era. In: The Globalization of Knowledge in History. Berlin: Max-Planck-Gesellschaft zur Förderung der Wissenschaften.
22.1 Introduction
In the volume Knowledge, Power, and Practice: The Anthropology of Medicine and Everyday Life Shirley Lindenbaum and Margaret Lock 1993have argued that the production and dissemination of biomedicine in societies worldwide has become inseparably intertwined with the social hierarchies, cultural mechanisms and moral, ethical and legal priorities prevailing in local and global power relations. In the context of modernization and globalization, the authors argue, the expansion of biomedicine cannot be thought of as being seperate from the way in which a more encompassing worldview and way of being is being enforced, produced and sustained. This is often achieved by marginalizing and rendering irrelevant other competing systems of (medical as well as non-medical) knowledge, practice and seeing the world.1
With regard to colonial Africa, Jean Comaroff 1993 has shown that the cultural legitimacy of biomedical knowledge was established not so much by emphasizing its scientific effectiveness and/or biomedicine’s pro-spective benefits for the colonized populations’ health, but rather by stressing biomedicine’s alleged moral superiority: Colonial bureaucrats and medical doctors propagated the idea that the acceptance of biomedically defined “healthy” lifestyles had become the necessary precondition for the social, moral and economic advancement of the colonized societies and for establishing a civilized and stable social order in the context of the colonial setup.2
Other chapters in Knowledge, Power, and Practice argue that the introduction and implementation of biomedical knowledge in various parts of the world has implied—and continues to imply—intense struggles over (health-related) meaning and practice on multiple levels of society, and the concurrent labeling and stereotyping of alternative forms of healing and religious, social and ritual practice as “traditional,” “backward” and “superstitious.” This latter view is often promoted not only by governmental and nongovernmental bodies and their representatives, but also by those parts of populations which identify themselves with “more educated” and “modern” worldviews. As Comaroff 1981 has argued, discourses on illness, healing and ritual are often more about the micropolitics of identity production than about specific persons and groups being “traditional” and/or “anti-modern.”3
The intimate relationship that exists between the production and circulation of biomedical knowledge and practice, on the one hand, and the establishment and perpetuation of globally and locally enforced worldviews, identities and power relations, on the other, has become nowhere more explicit than in the field of international development. The power dynamics that have been put in place by the globalized development framework over the last decades can be read in very different ways. One first version would be: Over the last twenty to thirty years, the economies and welfare systems of “Third World” countries have been reconfigured most drastically by reform programs imposed by the World Bank and the International Monetary Fund (IMF). From the late 1970s and early 1980s onwards such programs offered limited opportunities for national and local governing bodies and populations to negotiate well-being, knowledge and practices that contradicted the priorities and “urgency measures” dictated by international donors and development experts.4
However, while globalization and neoliberal reform processes have admittedly had a long-lasting effect on the political, social and economic configurations of many countries in the developing world,5 it would be an oversimplification to describe these processes exclusively with regard to the one-sided power relations that have shaped the positions of the “poor” and “rich,” “developed” and “underdeveloped” in a hierarchically structured world order. Thus, a second version of the history of international development would emphasize the fact that from the mid-1980s onwards international donors and development experts aimed not only at integrating local knowledge and expertise into the planning, organization and implementation of local development programs and projects. Development experts and project planners have also argued for actively decreasing the power hierarchies prevailing between the various “partners” involved in specific development projects in order to contribute “more effectively” to the material and social advancement of societies and populations in the developing world Green 2000. According to this latter view, “participatory approaches” in development imply the planning and implementation of projects and programs as the result of a process of mutual learning and interaction that is targeted first and foremost at the “empowerment” of local populations. As Maia Green puts it:
‘Development’ is not [then] simply a process of directed change leading to certain kinds of economic and social transformation, but depends on the accomplishment of a series of corresponding moral transformations in the consciousness of people participating, as change agents and changed, in the development process. Consequently, the proper task of development organizations and their personnel is to facilitate the necessary transformations in consciousness which can empower the poor as social actors to embark on locally managed change. Green 2000
While this is not the immediate focus of my chapter, it should be mentioned here that the ideals of “partnership” and “empowerment” are seldom translated into actual practice. Thus, a third way of interpreting the international development framework would highlight the fact that attempts at the realization of the partnership and empowerment paradigm have often led to paradoxical relations between actors in the field who, while often being critical or even cynical about the contradictions contained in development, ultimately affirm and reproduce the overall system Green 2000; Rottenburg 2009; Marsland 2006.
This chapter builds on all three approaches to globalization and development and looks at the way globally defined ideas about development, empowerment and knowledge production have been realized in the context of globalization processes of the last fifteen to twenty years in Tanzania, where development has become inseparably intertwined with neoliberal reform processes and the launching of structural adjustment programs in the country from the mid-1980s onwards. Focusing on the realm of HIV/AIDS programming and intervention, I will show that the multiple projects that have been established in the context of HIV-prevention, care and treatment programs—and the various types of knowledge these projects and programs produce and rely on—have become embedded in the global economy of aid, which has shaped the economic, social and cultural realities in wide parts of sub-Saharan Africa over the last decades. In particular, these programs and projects have focused on the promotion of “technologies of the self” and the production of subjectivities that rely strongly on the rationality and self-reflexivity of “empowered” individuals in forging appropriate and “healthy” ways of dealing with the disease.
The second part of the chapter will focus on some of the responses that rural and urban populations in Tanzania have articulated in relation to the HIV/AIDS epidemic and that have become intimately intertwined with people’s concerns about familial, social and economic developments in the context of modernity and globalization, and the moral and reproductive order at large. I argue that the implementation of “biopower” in rural and urban Tanzania, and thus, the production and circulation of biomedical knowledge in the neoliberal era, have to be understood as a fragmentary and contradictory process, which has become closely entangled with the way in which the global development industry is (re)creating zones and spaces of social service provision and health-related interventions in the East African region in the wake of neoliberal reform processes and emergent forms of globalizing humanitarianism.6 While biomedicine and processes of medicalization have played an important role in shaping individual and collective knowledge and behavior in relation to the disease in many parts of the continent, people are often simultaneously relying on alternative forms of knowledge and action in defining socially and morally appropriate ways of dealing with illness and death in the context of a transforming socio-moral and political order.
In the formulation of my argument, I rely strongly on my fieldwork in rural and urban Tanzania, which from 1995 onwards has explored different aspects of the interconnection between HIV/AIDS, knowledge production and social relationships in the context of globalization and modernity, including issues surrounding sexuality and gender relations, relationships of care and support, the moral management of AIDS-related illnesses and deaths, and recently the introduction of antiretroviral treatment, which has shaped health policy in Tanzania since the end of 2004.7
22.2 Governing Health in the Era of Structural Adjustment and HIV/AIDS
At the end of the 1970s, most countries in the Eastern and Southern African region stood on the verge of economic and political collapse. Governments were confronted not only with growing external debts and exploding costs in heavily subsidized economies and over-funded welfare systems, they were also struggling with the consequences of the international oil crisis and the global economic depression. All these factors combined drove many African governments to turn to the World Bank and the International Monetary Fund for assistance. The loans which were granted to African states by the World Bank and the IMF were intended primarily for use in stabilizing economies and paying-off national debts. However, they were also made contingent upon the implementation of a series of structural reforms in the respective countries which entailed, amongst others, currency devaluation, the reduction of trade barriers and the privatization of state-owned enterprises. Structural adjustment policies (SAPs) implied furthermore a steep reduction in governmental expenditure for healthcare, education and housing programs, including a drastic reduction of salary expenses for public sector employees.
The effects of structural adjustment on Tanzania’s healthcare sector were manifold. The former socialist country, which had banned private medical practice in 1977 in order to eliminate “profit thinking in the face of human suffering” Iliffe 1998, 209 reopened its healthcare system for private practitioners and health institutions in 1992 (ibid., 217). In 1999, there were already more than 500 private clinics and hospitals in Dar es Salaam alone Boller et.al. 2003, 117. In the year 2000 the government counted more than 1,270 private or religious dispensaries and 76 nongovernmental hospitals throughout the country.8 Cost-sharing programs, which were initially opposed by the former President Nyerere and his “socialist supporters”9 placed heavy burdens on patients and their families who, in addition to hospital and clinic charges, had to cover costs for transport, food, (admission) bribes, drugs and other medical supplies. In 2004, a report by the Women’s Dignity Project stated that “health care charges [in the country] have placed an impossible financial burden on the poorest households”; many fail to access primary care when they need it most and many more fail to obtain the necessary referral for more skilled care Mamdani and Bangser 2004, 151. Finally, the introduction of SAPs led to drastic cuts in state expenditures for the healthcare sector, and to an ever-growing reliance of Tanzania’s healthcare system on international and private funding to make up for the growing deficit: In 1990/1991, the national budget allocation for healthcare in Tanzania had fallen to 5% from 9.4% in the 1970s Harrington 1998, 149. In 2004, 49.9% of capital expenditure for the healthcare sector came from external sources; private expenditure on health, the largest share of which were out-of-pocket expenditures by patients and households (75.0%), amounted to 34.2%.10
The growing fragmentation and privatization of Tanzania’s public healthcare system—and the concurring influx of external funding into the country’s healthcare system—have become especially pervasive in the field of HIV/AIDS. Since the UN Declaration of Commitment on HIV/AIDS in 2001—and the subsequent launching of the Global Fund for the Fight Against AIDS, Tuberculosis and Malaria (2001) as well as the US Presidential Emergency Plan for AIDS Relief (PEPFAR) (2003)—international funding for the epidemic amounted in 2005 to more than eight billion US} on the global level. In Tanzania, financial resources for the fight against the epidemic increased steeply after the country was selected as one of the PEPFAR’s fifteen focus countries11: Under the Emergency Plan, Tanzania received more than 70.7 million US} in Fiscal Year (FY) 2004, nearly 108.8 million US} in FY 2005, and approximately 130 million US} in FY 2006 to support comprehensive HIV/AIDS prevention, treatment and care programs. In the years 2004/05 donor funding comprised 94.6% of the total public expenditure for HIV/AIDS and amounted to 377.8 billion Tanzanian shillings (ca. 219.6 million US$) during the same period TACAIDS 2008.
As in other countries in the sub-Saharan African region, international funding for HIV/AIDS in Tanzania is channeled partly through governmental institutions (in the case of treatment), and partly through the programs of NGOs, which have the reputation of providing transparent and accountable entry points for community-based development. In 2003, one NGO consultant in Dar es Salaam related that HIV/AIDS had become a “hot topic” in the country. Organizations that had not been involved in the topic so far were starting to engage in the fight against HIV/AIDS in order to attract additional funding; new NGOs were founded on a daily basis, existing sometimes only as “briefcase NGOs.” Finally there was growing competition between individual organizations aiming to develop new and innovative strategies of prevention, care and treatment in their constant struggles to attract donor money.
While the field of HIV/AIDS work has become increasingly complex and also short-lived, with many AIDS organizations attracting one or two-year funding commitments from a variety of mostly European and North American donors, HIV/AIDS-related programs have gradually subscribed to a focus on human rights and empowerment. This new type of intervention has placed the self-reflexive individual at the centre stage of HIV/AIDS-related policies and has granted the empowered actor with the capacity to deal responsibly and circumspectly with the risks associated with HIV infection and AIDS illness. To phrase it in the words of Michel Foucault the empowerment approach expects people to successfully apply
[…] technologies of the self, which permit individuals to effect by their own means or with the help of others a certain number of operations on their own bodies and souls, thoughts, conduct and way of being, so as to transform themselves in order to attain a certain state of happiness, purity, wisdom, perfection, or immortality. Foucault 1988, 18
To make sure, such an approach is not entirely new in the history of healthcare and healing in the wider Eastern and Southern African region, especially with regard to the field of mission medicine which was concerned explicitly with the formation of subjects. However, while subject formation has not been the focus of the wider, predominantly repressive power regime of the colonial state which was only marginally interested in the transformation of its citizens’ life worlds and individual and collective consciousness Vaughan 1991, the promotion of self-governing individuals in the post-colonial setting was constrained mostly to the level of health experts Langwick 2012 and did not rely on media and market forces to the extent it did in more recent decades. Furthermore, the more recent empowerment approaches are also different from earlier, information-based approaches in HIV prevention that were directed at an undifferentiated collectivity and often tried to make people fearful of possible infection with the deadly virus.
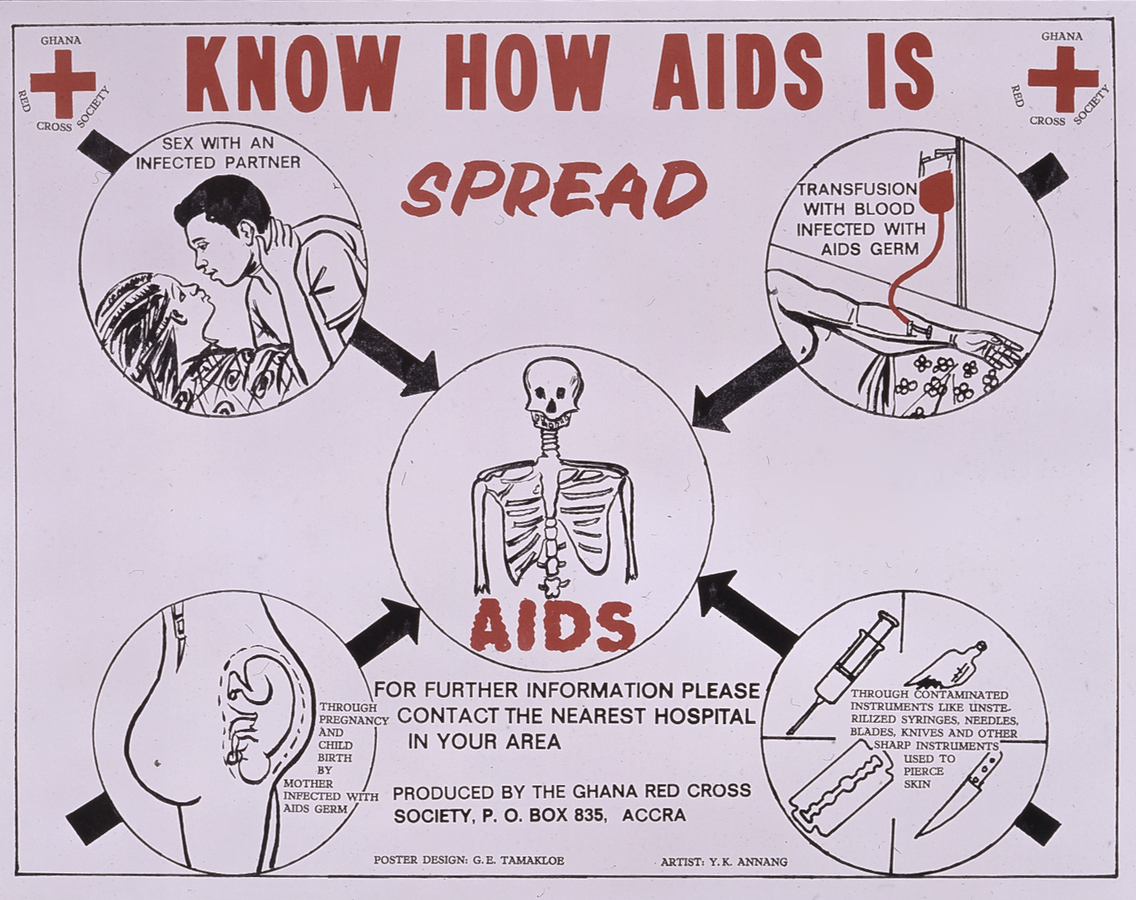
Fig. 22.1: AIDS Poster, Ghana Red Cross Society 1989. (Source: DeutschesHygiene Museum, Dresden)
Fig. 22.1: AIDS Poster, Ghana Red Cross Society 1989. (Source: DeutschesHygiene Museum, Dresden)
Fig. 22.2: Mural painting in Tanzania, 1999. (Photo: Dilger)
Fig. 22.2: Mural painting in Tanzania, 1999. (Photo: Dilger)
This “approach of deterrence,” as I would like to call it, is exemplified by the two figures below: Figure 22.1 represents a poster from Ghana from 1989 and displays a skeleton that is surrounded by messages concerning possible ways of HIV infection, thus scaring people about the deadly consequences of HIV. The same approach is used in a mural painting in Dar es Salaam (Figure 22.2) which simply states “AIDS is Death” (Ukimwi ni kifo) and, on the left, “Fear AIDS” (Ogopa ukimwi). Today, such generalized messages of deterrence have given way to empowering and participatory approaches, which have also gained ground in other areas of development work. In contrast with the earlier information-based approaches (including the “ABC approach” which relies on the tripartite message “Abstain, Be Faithful, or Use Condoms”12) the empowerment approach no longer simply tells people what to do or what not to do, i.e., how HIV is transmitted and what the consequences of risky behavior are in terms of infection and death. While such knowledge is implicitly contained in the “new” type of interventions, current prevention efforts are creating differentiated positions, which may be assumed in relation to HIV/AIDS, based on differences in age, gender, living environment, and also with regard to the professional and educational background of the respective target groups.
22.3 Technologies of the Self in “New” Approaches to Prevention, Care and Treatment
In Tanzania, technologies of the self in relation to HIV/AIDS policies are to be found most explicitly in prevention programs that focus on the growing urban middle class and that promote a discourse on “romantic” and “true” love among young people according to which partners talk openly about sexuality and birth control, as well as about protection from sexually transmitted diseases. This group of young people is sometimes called the “condom generation,” and in a broader sense it can indeed be understood as a reaction to the HIV/AIDS epidemic. The young men and women that are addressed by these interventions have become the target of a growing market of internationally-funded campaigns, which use different types of media interventions including talk shows, glossy magazines, counseling sections in newspapers, call-in radio shows etc., and which promote a view of sexuality that has become individualized and detached from family relations.
All these interventions targeted at young people are responding to the questions individual girls and boys may have about sexuality and HIV/AIDS. They offer advice with regard to specific life situations, which represent a risk in terms of HIV infection and, most importantly, they talk about the pleasures of sexuality. Thus, whereas earlier campaigns assumed that people know how to have sex and how to manage sexual relationships, this knowledge is no longer taken for granted and has to be negotiated.13 “True love,” as discussed and promoted by advice columns and picture stories run by fashionable lifestyle magazines, is based not solely on sexual attraction or satisfaction, but rather on values like friendship, loyalty, trust, respect and finally tenderness. The general message of such campaigns is that condoms are a sign of trust and mutual respect, not of mistrust or a way of blaming one’s partner for not being knowledgeable about sexuality and HIV.14 That this implies in turn an acknowledgement of responsibility to one’s self for one’s own health, and that safe sex can therefore be “cool” Posel 2005, 133 is expressed in the statement by twenty-two-year-old Shaban, the male character in a picture story run by Femina, a health journal for young people in Tanzania. He says:
If you want to be a winner in the game of love and pleasure, you have to go for condoms. Femina 2000, 25
On another level, technologies of the self have come to play a crucial role in the politics of “Living Positively” that have shaped HIV-positive identities all over sub-Saharan Africa during the last ten to fifteen years. Originating in Uganda in the early 1990s,15 this model provides a way for people with HIV/AIDS “to take care of their mind and body” and to enter into a “healthy relationship” with the life-threatening disease by a number of regulative practices and devices. These practices include the adherence to dietary requirements, regular medical checkups, the consistent treatment of opportunistic infections and finally the maintenance of social activities and regular exchange with others on dilemmas and problems associated with an HIV-infection. In Tanzania, this latter aspect has materialized in the form of numerous NGO support groups for people with HIV/AIDS, which provide a forum to discuss, negotiate and form opinions about various issues related to the illness. Topics discussed in the support group meetings in Dar es Salaam in 1999/2000, which took place on a regular basis and where people met three to four times per month, included disclosure and stigma, the challenge of balanced nutrition, “safe sexuality” in short- and long-term relationships, the lack of material support in times of illness, the writing of a will and the gains and disadvantages of traditional medicine.
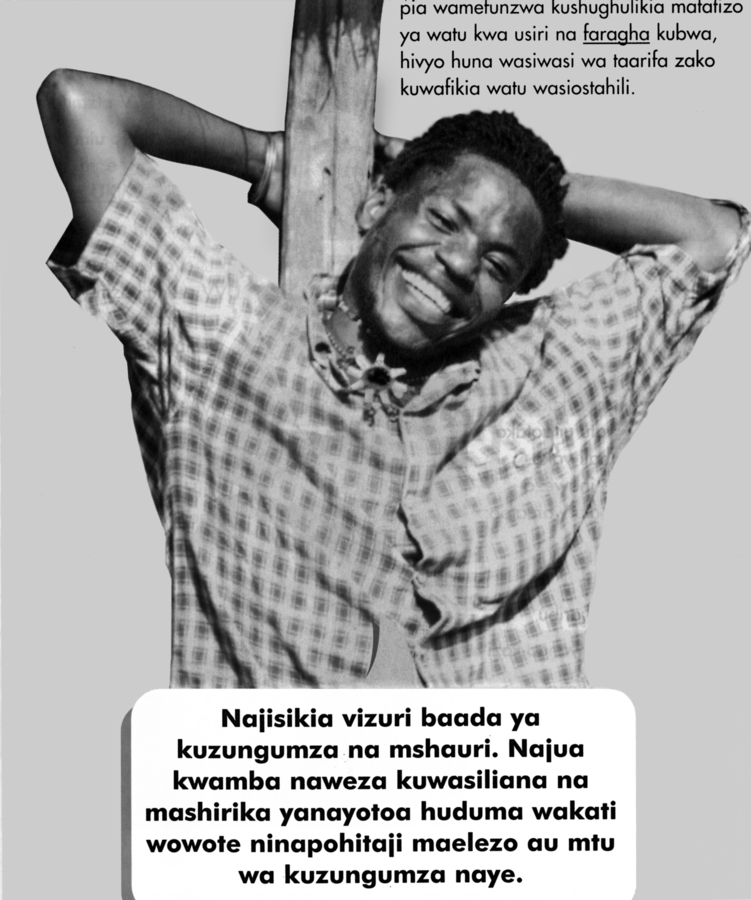
Fig. 22.3: The aspect of individual and collective counseling is addressed in images and stories of hope as presented in the booklet “Living Positively” (Kuishi kwa Tumaini: Living with Hope). The main character of the picture story displayed here is confronted with an HIV-positive diagnosis and—after going through a period of internal struggle and despair—has accepted his HIV-positive status. He says: “After I have talked to the counselor, I feel good. I know that I can talk to these organizations. They offer services whenever I am in need of advice or when I need a person to talk to.” The booklet “Living Positively with HIV” represents a good example of the way in which public health responses have become embedded in transnational channels of funding and knowledge production: The booklet has been adopted from the Soul City Institute for Health and Development Communication in South Africa and translated into Kiswahili and “culturally adapted to the Tanzanian setting” by the Health Information Project.(Femina, HIP, Tanzania)
Fig. 22.3: The aspect of individual and collective counseling is addressed in images and stories of hope as presented in the booklet “Living Positively” (Kuishi kwa Tumaini: Living with Hope). The main character of the picture story displayed here is confronted with an HIV-positive diagnosis and—after going through a period of internal struggle and despair—has accepted his HIV-positive status. He says: “After I have talked to the counselor, I feel good. I know that I can talk to these organizations. They offer services whenever I am in need of advice or when I need a person to talk to.” The booklet “Living Positively with HIV” represents a good example of the way in which public health responses have become embedded in transnational channels of funding and knowledge production: The booklet has been adopted from the Soul City Institute for Health and Development Communication in South Africa and translated into Kiswahili and “culturally adapted to the Tanzanian setting” by the Health Information Project.(Femina, HIP, Tanzania)
Beyond the pragmatic advice and the material aid provided by NGOs, the discussions in the support groups also fulfil a therapeutic function: It is through these extended conversations that people with HIV/AIDS (ideally) learn to accept their illness and to acquire a future-oriented and self-conscious approach to dealing with HIV. The information and advice given with regard to problems in partnerships, families or at the workplace is specific as well as generic and is becoming an essential part of the process of building a “positive identity,” despite experiences of grief, stigmatisation or despair about one’s material life circumstances (see Figure 22.3). Only few support group members I interviewed in Dar es Salaam were capable of initiating this healing process on their own. It was only through the repeated counselling and identification with the suffering of others that people adopted a self-image of being HIV-positive and translated this self-image into the context of marital and non-marital relationships, kinship networks and the wider community.
A final issue that has shaped the politics of HIV-positive identities in more recent years is the introduction of antiretroviral medications (ARV). ARVs have become available in Tanzania since the end of 2004. In collaboration with PEPFAR and the Global Fund, newly created treatment centres have been established all over the country. A number of booklets and handouts have been produced that stress the necessity of taking ARVs according to a fixed schedule and being aware of the importance of sticking to these drugs forever: “These expensive medicines,” reads one booklet which was adopted from the Soul City project in South Africa, “have to be taken every day, every month, your whole life.” Multi-coloured pamphlets call on people to observe their bodies carefully and to report unusual changes, symptoms and side effects to their physicians. ARVs are prescribed on a monthly basis and the dates of the last health clinic visit as well as the recommended return for check-ups are marked on a blue card that is used specifically for the prescription of ARVs and that allows people to visit other treatment centers around the country while traveling. Finally, the health planners see it as crucial for the success of ARV treatment that families and friends establish an open dialogue about these drugs in order to create a supportive environment for consistent and continuous drug regimens: “It is good to be with someone you trust,” reads one leaflet, “be it a relative or a friend, he will help you to remind you to take your medicine [as prescribed].” Thus, while people have been urged “to live positively with HIV” for more than a decade now, today they are required to “make a lifelong contract” with medications that have transformed the life-threatening disease into a chronic condition.
22.4 Beyond NGOs and “the Clinic”: Local Moral Worlds and the Limitations of Biopower in Tanzania
Looking at the numerous interventions that have been established in the field of HIV/AIDS over the last couple of years, one may wonder which particular “truths” about the disease (in the sense of Paula Treichler 1999) or, which type of “moral regimes” (in the Foucauldian sense), are being promoted by health programs in Tanzania that have evolved in the context of a market-driven, mostly nongovernmental and transnationalized response to the epidemic. In this section I want to argue that the empowerment approach—and the social, cultural and economic practices that are associated with it—are confined to specific settings; settings which can be described as “islands of biopower” that are sustained by the international AIDS industry which has based its activities increasingly on notions of human rights and self-responsibility and in recent years has aimed at the involvement of “affected communities” in its manifold activities.16
In medical anthropology, practices, ideals and technologies of the self, originating in the context of illness, health and well-being, in recent years have become closely related to discussions of biological citizenship; a form of citizenship that refers to the biological dimension of human life and “embodies a demand for particular protections, for the enactment or cessation of particular policies and actions [and for] access to special resources” Rose and Novas 2004, 441. In the context of HIV/AIDS, Vinh-Kim Nguyen 2005, 126 has subsumed the various practices, values and ideas that have emerged in the context of a globalized health response under the concept of therapeutic citizenship: a transnationalized form of biological citizenship, which makes claims on the global economic and social order based on a “shared therapeutic predicament.” According to Nguyen 2005, 125f., the social and cultural practices, which have evolved in this context over the last ten to fifteen years, have been organised around a complex set of confessional technologies and processes of self-fashioning. These are closely interwoven with internationally acclaimed forms of HIV/AIDS activism and essentially draw their legitimacy from the economic, political and biological inequalities existing in a globalizing world.
The practices and technologies of the self, which are evolving under these circumstances, can now be described with the concept of “biopower” which according to Foucault Foucault 1977 involves the exercise of power on a double, mutually intertwined level. On the individual level, the exercise of biopower presupposes a specific type of relationship with one’s body, as well as a specific type of subjectivity. Thus, whereas the exercise of state power is aiming at the regulation and control of the population as a whole, the exercise of individual power aims at the disciplining of one’s own body, the regulation of desire and the refashioning of the responsible sexual self. In this context, the care of one’s own health and body are intimately intertwined in that both are protected, cultivated and isolated from anything that is considered undesirable and dangerous. This creation of the “healthy self” through the application of technologies of truth and knowledge seems not dissimilar to the way in which the interventions of the mostly internationally funded AIDS-NGOs in Southern and Eastern Africa have come to present sexuality. According to Deborah Posel Posel 2005, 134 for AIDS NGOs—and certainly to some of their clients and target groups—sexuality has become a “site of rational, individual choice and agency, an opportunity for empowerment and ‘healthy positive living’.”
If we look now at the rural areas of Tanzania—and also beyond the context of NGOs and clinical settings in urban centers—we find that the ways people deal with HIV/AIDS are based as much on knowledge, discursive processes and technologies of the self that are derived from governmental and nongovernmental AIDS campaigns as they are embedded in the wider political economies of healthcare in Tanzania, and the social and moral priorities formulated by communities and families in relation to the disease. I want to illustrate this aspect briefly with regard to the ways families and communities in the rural Mara Region in Northwestern Tanzania—as well as in a Pentecostal congregation in Dar es Salaam—have come to deal with HIV/AIDS-related illnesses and deaths.17 While I focus on the ways in which people’s responses to HIV/AIDS have been shaped in specific settings of Tanzania beyond the NGO context, it should become clear that the processes and practices I describe here are not situated outside the globalized AIDS response and health sector in Tanzania. They have become inseparably intertwined with the processes described above in that they evolve in relation to the needs and challenges experienced in the wake of structural adjustment, privatization and the implication of Tanzania’s health system in transnationalized forms of governance. Furthermore, it has to be kept in mind that many of the HIV-positive women and men I encountered in Tanzania belong not only to one neatly bounded social entity or group, but identified themselves (sometimes only temporarily so) as NGO clients and/or church members along with their EOAemphasis on being part of one or more kinship networks.
22.4.1 Kinship, Care and Relatedness in Rural Mara
At the time of my research in the rural Mara Region in 1999/2000 governmental and nongovernmental care programs were established only in rudimentary ways.18 The expensive care and treatment provided by local private hospitals was affordable to only a few rural families, who lived primarily from agriculture and petty trade, in part from fishing and from the support of family members who were living and working in the cities. Relationships of care and support in this context were shifted out of necessity to the families with members with HIV/AIDS and were embedded, amongst others, in family conflicts, the beginnings of which often existed long before the outbreak of illness. Especially with regard to sick relatives from cities like Dar es Salaam, Mwanza or Arusha, family tensions had an effect on situations of care provision as sick relatives who had been living in the city often returned unwillingly to their home villages under pressure from their (urban) relatives. On the other hand, the return of these relatives, who in some cases had paid little attention to the well-being of their rural families during preceding years, presented a significant economic, social and emotional strain for their rural family members Dilger 2005; Dilger 2006; Dilger 2008.
In addition to the internal family conflicts and significant social and economic difficulties the care of family members sick with AIDS in a rural setting implied, the differences in the quality of care and the availability of the care provided was determined above all by gender specific dynamics. The latter played a particularly important role with regard to the care situations of young women. In the patrilineal family structures of the research region, women and their children were considered part of the husbands’ families following marriage. As such, their care in times of sickness or in the case of the death of their husbands was considered the responsibility of their husbands’ relatives. In reality, however, these rules and expectations often represented the basis for tension and discussion across family networks: in particular with regard to young wives who became ill with HIV/AIDS, the question would be raised if they were “properly” married and if the marriage had been “correctly” confirmed through a dowry. Discussions concerning proper marriages—and thus the recognition of the status of a wife—were especially common concerning childless women as well as widows, whose claims on their husbands’ inheritances would be shared not only with their children, but with their in-laws as well.19
On another level, relationships of care and support were shaped by the kinship-based politics of burial and belonging, which forced people who had worked and lived outside of their villages for extended periods to return to their rural homes when death was approaching. Questions concerning care and the subsequent burial—and especially the place of burial—were thereby potentially conflictive questions and reflected again on the dynamics of age, gender and belonging within patrilineal kinship networks.20 Thus, while in some cases the care and the burial of male relatives raised questions concerning (unfulfilled) solidarity and kinship obligations, the situation of women was often more troubling to the families involved. Especially in the case of younger women who had been married to their husbands only recently and who had no children, or only a few at the time of their death, the question was posed to which family they actually belonged and who was responsible for their care and burial: their husband’s or their father’s family. Unmarried (or not formally married) women, on the other hand, were cared for mostly by their family of origin and buried on the compound of their brother-in-law who thus provided the deceased with the status of a co-wife.21
Finally, prior to the arrival of ARV the families in rural Mara dealt with HIV/AIDS illnesses by keeping silent about the infections and deaths of family members. Prior to the arrival of ARV, only very few HIV-infected men and women among my informants knew about their diagnosis and hardly any of them talked openly about it. Testing and counseling was carried out in the local hospitals, but only for those patients who were suspected to have been infected with HIV by the health staff. Those patients who were found to be HIV-positive were often not informed about their diagnoses, and those who were, were sent home due to the high costs of nursing AIDS patients and due to beds in the local hospitals becoming increasingly over-occupied. However, while at the turn of the century the silence on the biological dimensions of the disease had become for people in Mara an integral part of referring to illnesses and deaths in the time of AIDS, this did not mean that there was no talk at all about the illnesses of dying community members or relatives. On the one hand, HIV/AIDS-related illnesses and deaths were the subject of multiple rumors that were circulating in the villages and that concerned the nature and origin of suffering—as well as the sexual relationships and networks that were its alleged root cause—in detail. The targets of this talk were carefully trying to prevent these rumors from spreading—sometimes even beyond death—and many people were hesitant to discuss their claims openly, especially if the person who was suspected of an HIV infection was a powerful and influential member of the community.
On the other hand, many individuals and families in Mara referred to HIV/AIDS in terms of other diseases such as tuberculosis or herpes zooster, or associated it with witchcraft and also chira, a disease that was said to be caused by the non-observance of ritual prescriptions, the symptoms of which were described as being very similar to AIDS Dilger 2006; Dilger 2008. While at the time of my research not all people in Mara would have argued that all cases of HIV/AIDS were related to chira, in those cases where the connection was established this had immediate effects on the way treatment was sought for patients and how care and support were being organized within family networks (this being related essentially to the fact that chira was said to be curable with the help of local herbs).
22.4.2 Healing, Community and Care in a Neo-Pentecostal Congregation in Dar es Salaam
In rural areas as in urban centers of Tanzania the daily lives of people living with HIV/AIDS are often more complex than public health programs suggest. In particular in Dar es Salaam, Neopentecostal churches, which have seen drastic increases in the number of members in large sections of sub-Saharan Africa in recent years, have played an important role in the social, economic and religious life situations of people with HIV/AIDS. The Full Gospel Bible Fellowship Church (FGBFC) in Dar es Salaam in which I conducted fieldwork in 1999 and 2000 was founded in 1989 by Zachariah Kakobe, a charismatic bishop from Southern Tanzania who had earned his living as a musician and meteorologist before receiving his calling in 1980. Over the last twenty years, the church has established branches in almost all regions and districts of the country and counted more than 120,000 members nationwide in the year 2000. In 1999, the FGBFC caused a stir through its public AIDS healings, which attracted 300–400 people a week and were hotly debated in the print media and among the public.22
For the members of the FGBFC I encountered during my fieldwork, the church became a source of hope mainly through its gospel of prosperity and, intimately related to it, the concepts of “awakening” and “salvation.” According to Corten and Marshall-Fratani 2001 salvation in a Pentecostal church is “an ongoing existential project,” which requires engagement in church activities and healing prayers in order to ward off attacks by diabolic forces as well as a break with many of the obligations church followers have towards their families (especially the “cultural” and “ritual” obligations which are associated with the central phases of life, i.e. birth, marriage and death).23 In the case of the FGBFC, the church teachings required furthermore the abandonment of sinful lifestyles such as consumption of alcohol or engagement in extramarital sexual relationships. It was only if these (admittedly difficult) conditions were fulfilled that the manifold promises of salvation began to work in multiple directions. Thus, the gospel of health and wealth in the FGBFC promised not only material success and progress for those living in poverty. Salvation also meant the relief from all kinds of distress such as trouble at work or with the Tanzanian bureaucratic system, as well as from diseases such as infertility, cancer, high blood pressure or AIDS.24
Apart from the AIDS healings, which according to the church’s bishop and his followers have been confirmed in some cases by biomedical tests, the church has established a network of mutual solidarity that provides help and support for members in times of need and crisis. At the time of my research, the church had established a dense network of small neighbourhood churches which comprised twenty to thirty members each and in which the idea of a “spiritual family” was promoted. This was defined in opposition to the worldly family and aimed to build a new moral community that was to disperse any doubts the church members might have about the righteousness of their path. This process of relation and community building was an ambiguous process which implied a high potential for intra-familial conflict, stemming both from unsaved relatives who tried to make church members depart from the path of salvation, as well as from the church followers who persistently urged their families to give up their “dark” and “sinful” ways. However, the FGBFC was described to me by its members not only as a source of conflict, but also as a beneficial network of care and support that flexibly reacted to the needs of its individual followers. Especially in cases of serious illness the charitable acts of other church followers went far beyond immediate acts of caring or nursing and often included arrangements of funerals, etc. The provision of such acts of solidarity had become particularly beneficial for the mostly female members of the church who were mainly young to middle-aged women with low educational status who had migrated to Dar es Salaam in search of employment or business opportunities during the 1980s or 1990s. To these women—as well as to the male members of the church most of whom had a similar social background—the FGBFC was appealing essentially because it offered a space of hope, stability and moral orientation in the urban context, which was experienced as increasingly risky and ambivalent.
What can be drawn now from these two case studies on the FGBFC and on kinship networks in rural Mara? As I hope to have shown, there may be significant gaps between what the “empowered individuals” of transnationally designed health programs—including subjects formulated predominantly by NGOs—and people who perceive of themselves mainly as members of kinship and other community-based networks “know” about illness and well-being in the times of AIDS. People in Tanzania, who may have a range of resources at their disposal and who may depend in their decisions on a variety of social and cultural settings and relationships do not always act in accordance with public health messages or with regard to the greatest benefits to their own (or others’) biologically-defined health. At the turn of the century, individual and collective behaviors in the era of AIDS were not only constrained by growing economic pressures and the lack of access to healthcare services, which had been triggered by neoliberal economics and political reforms in the health sector over the previous two decades. They were also rooted in the logics of community and kinship politics and in the moral, cultural and religious priorities that people had with regard to the persistence of social relationships in and beyond the context of death and suffering. The exclusive focus on lifeworlds that are promoted and represented by state actors, nongovernmental organizations and humanitarian interventions would have revealed only a partial view of the complex social and cultural processes that have come to shape the knowledge, experience and practice surrounding HIV/AIDS in Tanzania and other parts of sub-Saharan Africa. Consequently, I would argue that if we think critically about notions of citizenship and self-care in relation to HIV/AIDS, we need to take account of the complex relationships between power, experience and practice which have shaped people’s identities and subjectivities in the wake of globalization and the emerging epidemic.
22.5 Conclusion: Knowledge, Practice and (Bio)Power in the Context of Globalization
In the course of doing fieldwork in Tanzania, I was often struck by the fact that while people were generally well aware of how HIV is transmitted, how to protect oneself from infection, or how one should supposedly behave towards people with HIV/AIDS, their actual behaviors concerning sexuality or HIV/AIDS-related illnesses and deaths were often directly opposed to this information. Thus, while health messages about HIV/AIDS were widely acknowledged among people in Tanzania even before the introduction of antiretroviral treatment, social and cultural practices surrounding sexuality or episodes of HIV/AIDS-related illnesses and deaths were shaped less by information and knowledge drawn from governmental or nongovernmental HIV/AIDS programs, but had become intimately intertwined with people’s concerns about familial, social and economic developments in the context of modernity and globalization, and the moral and reproductive order at large. The few examples I have given in the previous section should suffice to state that over the last two decades individual and collective behaviors in the era of AIDS have not only been constrained by growing economic pressure and uncertainties triggered by neoliberal economics and political reforms. They are also rooted in the logics of community and kinship politics and in the moral, cultural and religious priorities that people have with regard to the persistence of social relationships in the context of death and suffering.25
In contrasting the different ways in which individuals, families, communities and a wide range of governmental and nongovernmental actors have come to deal with HIV/AIDS in rural and urban Tanzania, three issues are interesting to observe. All of these issues shed light on the way in which the relation between knowledge, practice and (bio)power has been shaped and reconfigured in the context of globalization and neoliberal reform processes over the last two decades. First, the analysis above has made clear that the various contexts in which people have come to act on HIV/AIDS in Tanzania imply shifting understandings of the causal connection between knowledge and practice. While earlier approaches in HIV/AIDS prevention were based on the “rational actor model” and have assumed that the availability of knowledge (in the sense of information) translates necessarily into practice (in the sense of behavior), more recent approaches have adopted a broader view of this connection. Thus, approaches that are based on the notion of empowerment acknowledge that biomedical and public health knowledge acquire meaning only in relation to the larger contexts in which individual behavior is supposed to materialize. Addressed are in particular the (gendered) relationships between sexual partners, emotional states like fear, love or hope, the dynamics in (nuclear) families, and—to a minor extent, the socio-economic and legal conditions that shape the lives of individual actors in contemporary Tanzania. Excluded remain, however, the larger transformations in politics and healthcare in the country, alternative notions of illness and healing, and also the dynamics of kinship and belonging in relation to extended family networks and religious communities in urban and rural settings. As argued above, these latter aspects play a crucial role in shaping individual and collective behaviors and practices in relation to HIV/AIDS in rural and urban areas.
Second, the different types of knowledge, practice and experience that have emerged in the context of globalization and HIV/AIDS in Tanzania are inseparably intertwined with different types of subjectivities and the reflexive self which are in turn built around shifting concepts of the person and gender. Thus, the approaches and interventions of nongovernmental organizations perceive of their target groups and clients as largely autonomously acting individuals who, in the case of women, need to be empowered socially, economically and legally in order to be able to make healthy and responsible decisions. Men, on the other hand, are seen as economically, socially and legally privileged and as being largely in charge of most of the decisions relating to their partnerships and families. Only in recent years have NGOs and local interest groups come to reflect critically on socially constructed modes of masculinity and male sexuality and have emphasized the need for men’s “cultural empowerment,” which might enable them to assume a “positive” gender role as responsible husband, son, father and sexual partner.26
Such discourses and images contrast with the expectations, roles and responsibilities that are formulated for the behaviors of men and women in other areas of life in Tanzania. In the patrilineal kinship networks in rural areas, the well-being of individual men and women is often closely interwoven with the fate of their—and in the case of women their husbands’—nuclear and extended families. Illness and suffering are often understood here as a reflection of the wider state of (gender and age-specific) social relations which are perceived as being disturbed by globalization and migratory processes and which need to be worked upon in order to ensure individual and collective well-being. In contrast, Pentecostal churches like the FGBFC in Dar es Salaam, offer new spaces of solidarity and attachment—especially for women—and thus provide an alternative to the male-centred kinship networks of rural and urban areas. Such churches often pursue a highly conservative gender ideology, however, which is centred on the nuclear family and which expects decency and submissiveness of women towards their husbands. It is important to emphasize that these different types of gendered subjectivities and concepts of the person as outlined here are not mutually exclusive. People’s lives are often shaped in relation to different urban as well as rural localities and social settings through which they are exposed to shifting, and often conflicting, types of expectations, knowledge and values.
Finally, the way knowledge, truth and meaning are produced and reproduced in relation to HIV/AIDS in various settings of Tanzania has been shaped by the context of global development and health restructuring over the last two to three decades, as well as by the multiple iconographies and textual representations that have become part and parcel of the process of producing meaning and truth in the era of globalization. On the one hand, globally driven development precludes the integration of certain types of truth and knowledge into health interventions, a fact that is amply illustrated by the various images, texts and statistics produced by governmental as well as nongovernmental actors in the form of flyers, booklets and reports. In particular, the multiple moral conflicts relating to decisions concerning health and sexuality—but also people’s alternative knowledge and experiences concerning illness, healing, death and mourning—are seldom addressed by internationally funded interventions and programs. Thus, while “local knowledge” and experiences are highly valued in other areas of development work in Tanzania (especially in agriculture and more recently also in the field of traditional medicine), HIV/AIDS interventions in the country have often engaged a modernizing approach that reproduces established dichotomies like “tradition vs. modernity,” “belief vs. knowledge” and “religion vs. medicine and science.” In this context, local knowledge, experience and practice, which have become partially represented in local Swahili publications and cartoons, are often branded as “superstitious,” “harmful” and “backwards.”
On another level, and related to this, the production and dissemination of knowledge, meaning and truth in the neoliberal era have been shaped by the growing disjuncture between the practices, experiences and ideas of (internally further differentiated) families and communities, on the one hand, and the expectations and values that are promoted by the (equally differentiated) HIV/AIDS industry, on the other. Thus, this text has shown that the promises and services of NGOs and FBOs have had an impact on the lives of many individuals, some of whom have benefited from the new funding arrangements that have also opened up new avenues into the globalized health order on a personal level. Many others, however, rely on knowledge and relationships beyond the biomedically defined health settings, and try to act on their bodies and illnesses by drawing on a wide range of resources that have emerged, and have been transformed, in response to HIV/AIDS and shifting social and political-economic conditions. In conclusion, I would like to argue therefore that this disjuncture has become reflective of the way in which the circulation of medicine and biopower in the neoliberal era has been shaped by the way global capital and development are “hopping” over sub-Saharan Africa Ferguson 2006 thereby reconfiguring social, economic and cultural constellations on the continent in only fragmentary ways. Thus, while the production and spreading of biopower in Tanzania have become embedded in globalized channels of funding, which govern “regimes of truth and knowledge” in the context of HIV/AIDS and structural adjustment in often contradictory ways, the state and its institutions—as well as the nongovernmental actors that have become complementary to them—have only limited ability to establish and exercise biopolitical authority in a pervasive way. Under these conditions, many Tanzanians have developed a critical sense of their government’s ability to control the living conditions of its citizens on a daily basis, thus looking for “collective solidarity” and “moral beneficence outside of the state altogether” Ferguson 2006, 85. In this regard, moral knowledge, practice and experience—and the various forms of sociality and belonging that have been built around them—have remained of crucial importance to individuals, communities and families in making sense of the transformations and challenges related to globalization and responding actively to the suffering associated with HIV/AIDS.
References
Boller, Christoph, Kaspar Wyss, K. W., Mtasiwa Kaspar (2003). Quality and Comparison of Antenatal Care in Public and Private Providers in the United Republic of Tanzania. Bulletin of the World Health Organization 81(2): 116-122
Cohen, David William, E. S. Atieno Odhiambo (1992). Burying SM: The Politics of Knowledge and the Sociology of Power in Africa. Portsmouth, NH: Heinemann.
Comaroff, Jean (1981). Healing and Cultural Transformation: The Tswana of Southern Africa. Social Science and Medicine 15b: 367-387
- (1993). The Diseased Heart of Africa: Medicine, Colonialism, and the Black Body. In: Knowledge, Power, and Practice: The Anthropology of Medicine and Everyday Life Ed. by Shirley Lindenbaum, Margaret Lock. Berkeley, CA: University of California Press 305-329
Corten, André, Ruth Marshall-Fratani (2001). Introduction. In: Between Babel and Pentecost: Transnational Pentecostalism in Africa and Latin America Ed. by André Corten, Ruth Marshall-Fratani. Bloomington, Ind.: Indiana University Press 1-21
Dilger, Hansjörg (2001). Living PositHIVely in Tanzania: The Global Dynamics of AIDS and the Meaning of Religion for International and Local AIDS Work. Afrika Spectrum 36(1): 73-90
- (2003). Sexuality, AIDS and the Lures of Modernity: Reflexivity and Morality among Young People in Rural Tanzania. Medical Anthropology 22(1): 23-52
- (2005). Leben mit Aids: Krankheit, Tod und soziale Beziehungen in Afrika; eine Ethnographie. Frankfurt am Main: Campus.
- (2006). The Power of AIDS: Kinship, Mobility and the Valuing of Social and Ritual Relationships in Tanzania. African Journal of AIDS Research 5(2): 109-121
- (2007). Healing the Wounds of Modernity: Community, Salvation and Care in a Neo-Pentecostal Church in Dar es Salaam, Tanzania. Journal of Religion in Africa 37(1): 59-83
- (2008). “We Are All Going to Die”: Kinship, Belonging and the Morality of HIV/AIDS-Related Illnesses and Deaths in Rural Tanzania. Anthropological Quarterly 81(1): 207-232
- (2012). Targeting the Empowered Individual: Transnational Policy-Making, the Global Economy of Aid, and the Limitation of `Biopower' in the Neoliberal Era. In: Medicine, Mobility, and Power in Global Africa: Transnational Health and Healing Ed. by H. Dilger, A. Kane, A. K.. Bloomington, Ind.: Indiana University Press
Dilger, Hansjörg, Ute Luig (2010). Morality, Hope and Grief: Anthropologies of AIDS in Africa. Oxford: Berghahn Books.
Escobar, Arturo (1995). Encountering Development: The Making and Unmaking of the Third World. Princeton, NJ: Princeton University Press.
Femina (2000) Femina HIP, February–April 2000, Tanzania.
Ferguson, James (2006). Global Shadows: Africa in the Neoliberal World Order. Durham, NC: Duke University Press.
- (2007). The Anti-Politics Machine: “Development”, Depoliticization and Bureaucratic Power in Lesotho. Minneapolis, Minn.: University of Minnesota Press.
Foucault, Michel (1977). Der Wille zum Wissen. Frankfurt am Main: Suhrkamp.
- (1988). Technologies of the Self. In: Technologies of the Self: A Seminar with Michel Foucault Ed. by Luther H. Martin, Huck Gutman, H. G.. Amherst, Mass.: University of Massachusetts Press 16-49
Frontières, Medecins Sans (2010). No Time to Quit. Médecins Sans Frontières: Brussels Operational Centre.
Green, Maia (2000). Participatory Development and the Appropriation of Agency in Southern Tanzania. Critique of Anthropology 20(1): 67-89
Harrington, John A. (1998). Privatizing Scarcity: Civil Liability and Health Care in Tanzania. Journal of African Law 42(2): 147-171
Heald, Suzette (2002). It's Never as Easy as ABC: Understandings of AIDS in Botswana. African Journal of AIDS Research 1(1): 1-10
Iliffe, John (1998). East African Doctors: A History of the Modern Profession. Cambridge: Cambridge University Press.
Langwick, Stacey (2012). The Choreography of Global Subjection: The Traditional Birth Attendant in Contemporary Configurations of World Health. In: Medicine, Mobility, and Power in Global Africa: Transnational Health and Healing Ed. by H. Dilger, A. Kane, A. K.. Bloomington, Ind.: Indiana University Press
Lindenbaum, Shirley, Margaret Lock (1993). Knowledge, Power and Practice: The Anthropology of Medicine and Everyday Life. Berkeley, CA: University of California Press.
Mamdani, Masuma, Maggie Bangser (2004). Poor People's Experiences of Health Services in Tanzania: A Literature Review. Reproductive Health Matters 12(24): 138-153
Marsland, Rebecca (2006). Community Participation the Tanzanian Way: Conceptual Contiguity or Power Struggle?. Oxford Development Studies 34(1): 65-79
Meyer, Birgit (1998). `Make a Complete Break with the Past.' Memory and Postcolonial Modernity in Ghanaian Pentecostal Discourse. In: Memory and the Postcolony: African Anthropology and the Critique of Power Ed. by Richard Werbner. Postcolonial Encounters Series. London: Zed Books 182-208
Morrell, Robert (2001). Introduction: The Times of Change. Men and Masculinity in South Africa. In: Changing Men in Southern Africa Ed. by Robert Morrell. Pietermaritzburg: University of Natal Press 3-34
Nguyen, Vinh-Kim (2005). Antiretrovirals, Globalism, Biopolitics, and Therapeutic Citizenship. In: Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems Ed. by Aihwa Ong, Stephen J. Collier. Oxford: Blackwell 124-145
Parikh, Shanti A. (2005). From Auntie to Disco: The Bifurcation of Risk and Pleasure in Sex Education in Uganda. In: Sex in Development: Science, Sexuality and Morality in Global Perspective Ed. by Vincanne Adams, Stacy Leigh Pigg. Durham, NC: Duke University Press 125-158
Pigg, Stacy Leigh (2002). Too Bold, Too Hot: Crossing `Culture' in AIDS Prevention in Nepal. In: New Horizons in Medical Anthropology: Essays in Honour of Charles Leslie Ed. by Mark Nichter, Margaret Lock. New York: Routledge 58-80
Posel, Deborah (2005). Sex, Death and the Fate of the Nation: Reflections on the Politicization of Sexuality in Post-Apartheid South Africa. Africa: Journal of the International African Institute 75(2): 125-153
Rose, Nikolas, Carlos Novas (2004). Biological Citizenship. In: Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems Ed. by Aihwa Ong, Stephen Collier. Oxford: Blackwell Publishing
Rottenburg, Richard (2009). Far-fetched Facts: A Parable of Development Aid. Cambridge, Mass.: MIT Press.
TACAIDS (2008) Tanzania Public Expenditure Review. Multi-Sectoral Review: HIV-AIDS December 2007.
Treichler, Paula A. (1999). How to Have Theory in an Epidemic: Cultural Chronicles of AIDS. Durham, NC: Duke University Press.
Vaughan, Megan (1991). Curing Their Ills: Colonial Power and African Illness. Cambridge: Polity Press.
Whyte, Susan Reynolds (2005). Going Home? Belonging and Burial in the Era of AIDS. Africa: Journal of the International African Institute 75(2): 154-172
- (2009). Health Identities and Subjectivities: The Ethnographic Challenge. Medical Anthropology Quarterly 23(1): 6-15
Whyte, Susan Reynolds, Michael A. Whyte, M.A. W. (2010). Health Workers Entangled: Confidentiality and Certification. In: Morality, Hope and Grief. Anthropologies of AIDS in Africa Ed. by Hansjörg Dilger, Ute Luig. Oxford: Berghahn Books
Among PEPFAR’s fifteen focus countries, which represent collectively approximately 50% of HIV infections worldwide, are five Eastern African countries: Ethiopia, Kenya, Rwanda, Tanzania and Uganda.
While my critique of concepts like “biological” or “therapeutic citizenship” in this section focuses mostly on settings and relationships situated outside of NGOs and biomedical institutions, the validity of these concepts has also to be questioned for the context of NGOs itself as well as for the biomedical sector in general. Thus, as Whyte 2009 and Whyte et.al. 2010 have argued, the rollout of antiretroviral medications raises challenging questions for anthropological debates on ethics, subject formation and understandings of biological and/or therapeutic citizenship. These questions may become even more pertinent with the current cutbacks in global funding for antiretroviral treatment and the impact this may have on the accessibility of local and national treatment programs Frontières 2010. Furthermore, the confines of this article do not allow me to elaborate on the manifold social and cultural processes influencing not only the domains of care and illness experience, but also sexuality in rural Tanzania. Thus, while a discourse on “true love” is taking place even in rural areas, other aspects such as inequality between the sexes, the significance of gifts and money for sexuality, as well as concepts of moral integrity and sexual pleasure are just as essential for the shaping of sexual relationships of young men and women as the knowledge being conveyed by national and international campaigns. Cf. Dilger 2003.
In the year 2001 around 9% of the region’s adult population was infected with HIV. However, there had been no continuous HIV/AIDS response in the villages until 2005 when an ARV treatment center was put in place by the government in collaboration with one of the private, mission-based hospitals in the area.
On the liminal situation of (young) women in patrilineal kinship networks in Uganda, and the challenges this liminality entails for their burials in the time of AIDS, see Whyte 2005. In Western Mara, conflicts and discussions concerning the burials of men and women in the context of HIV/AIDS were also driven by the concern that the spirit of a deceased person might seek revenge if ritual prescriptions were not observed. The danger was considered especially high from women or young girls who were not married at the time of their death. If they were buried within their father’s compound they were said to attract evil spirits and unleash infertility among their female relatives.